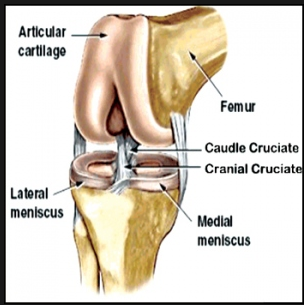
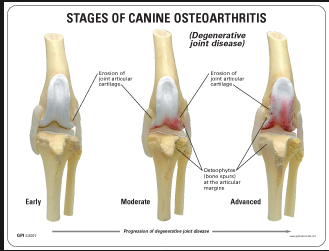
Normal Knee
The two most common knee problems encountered in veterinary practice today are Anterior Cruciate Ligament Ruptures and Medial Patella Luxations. For discussions concerning fractures of the knee, please refer to the fracture section.
When should I have my dogs ACL evaluated?
- If your dog is limping on one or even favoring both hind limbs.
- If your dog is sitting down different with one rear leg extending out or pulled under the body.
- If your dog becomes lame after exercise.
- If your dog is slow to rise after resting for a period of time.
- If your dog is reluctant to run, jump, or play normally.
- Anterior cruciate ligament (ACL), also known as Cranial Cruciate Ligament (CCL), injury is one of the most common causes of rear limb lameness seen in veterinary practice today.
- The ACL is responsible for maintaining joint stability and preventing tibial thrust.
- Once torn, the tibia is allowed to thrust forward during the weight bearing motion of the rear limb, causing pain and a moderate to severe limp.
- Another secondary problem commonly associated with ACL tears is medial, and less commonly, lateral meniscal tears which compounds the problems and increases the discomfort and degree of lameness seen in the canine patient.
- ACL injuries can occur in all sizes of animals ranging from small to giant.
- Tears of the ACL can range from complete rupture to a partial tear, with some partial tears being almost impossible to detect clinically. This is where MRI scanning can greatly improve the speed and accuracy of partial tear detection.
- Early detection of a tear is vital for the best possible return of function after surgical correction. By correcting ACL tears sooner, we can return you pet to a better quality of life and reduce the amount of time your animal has to be in pain from this condition.
- We recommend that all animals with a complete or partial ACL tear undergo an MRI evaluation to assess the meniscal and cartilage health of the knee. This greatly improves our ability to correctly identify meniscal problems so they can be addressed properly during surgery.
Two ACL Surgical Options:
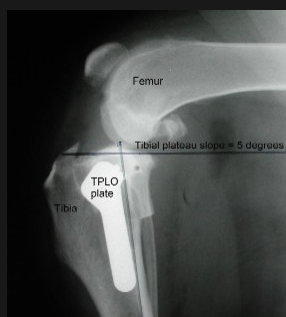
Tibial Plateau Leveling Osteotomy (TPLO)
- TPLO currently the gold standard for ACL repair for dogs weighting 45 pounds and over.
- A TPLO is a corrective osteotomy that eliminates tibial thrust in the ACL deficient knee by changing the angle of the tibial plateau in relation to the femur.
- After a TPLO, most animals experience a return of function that can reach 90-93% of normal.
- This level of return of function is unmatched by any other Extra- Capsular techniques.
Healing time after a TPLO is 6-8 weeks, followed by a 2-3 month rehabilitation period which is done at home under owner supervision.
-

- Post-Op Radiograph TPLO
-
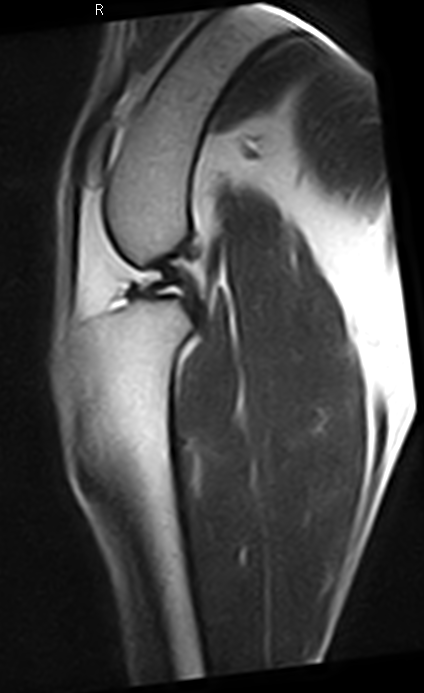
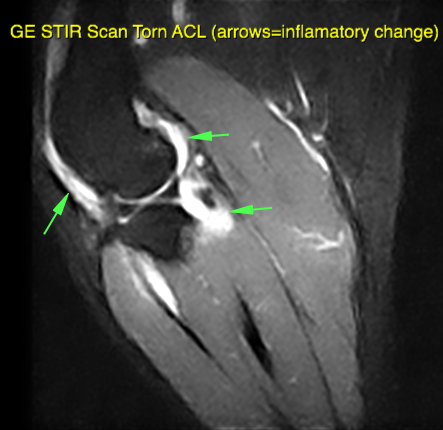
- MRI Torn ACL
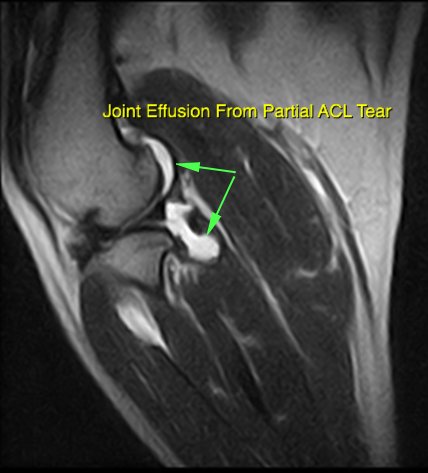
-
- MRI Torn ACL
-

- Lateral Meniscal Tear

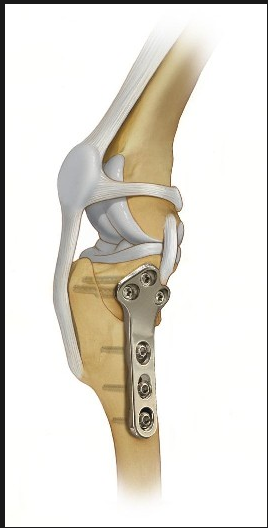
Extra-Capsular Repair
- This technique employs an implant that is placed outside the joint capsule.
- This surgery is designed to decrease tibial thrust by giving external support to the joint.
- The implants are designed to maintain tensile strength for up to 6-8 months after surgery, allowing time for scar tissue to form which supports and stabilizes the joint long term.
- Although this technique does not provide the stability that a TPLO does, it is still considered a viable option for repair.
- Extra-Capsular repair is the technique of choice for most small dogs weighting less then 45 pounds.
Medial Patella (Knee Cap) Luxation
Medial patella luxation is a one of the most common knee abnormalities diagnosed in veterinary practice today. 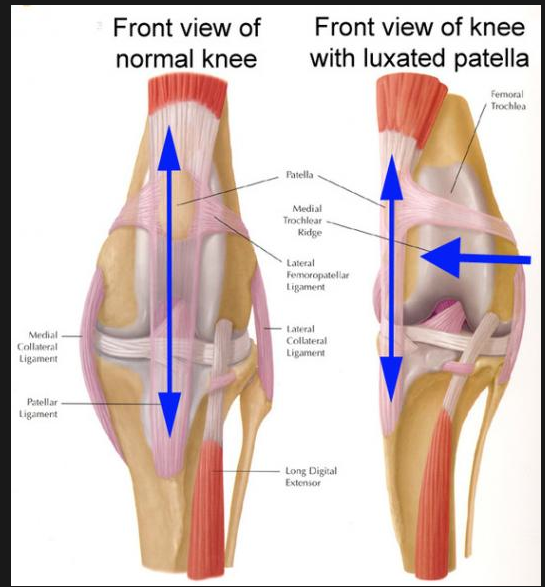 Although most commonly diagnosed in small dogs, it has become more increasingly found in medium to large breed as well. The condition is described as the loss of the ability to keep the patella (knee cap) in the femoral groove. There are four grades of medial patella luxation.
Although most commonly diagnosed in small dogs, it has become more increasingly found in medium to large breed as well. The condition is described as the loss of the ability to keep the patella (knee cap) in the femoral groove. There are four grades of medial patella luxation.
- The knee cap can be luxated by the examiner manually but reduces back in on its own.
- The knee cap luxates on its own but is in the correct anatomical position most of the time.
- The knee cap is luxated out of place most of the time but can be put back into normal anatomical location by the examiner manually.
- The knee cap is luxated permanently and can not be reduced to a normal anatomical location manually.
We recommend surgical correction for grade 3, 4 luxation and some grade 2 luxations, if they are causing clinical lameness. Grade 4 luxations have the worst surgical prognosis because of the severity of the condition.